New 2026 Cholesterol Recommendations: comprehensive analysis and comparison with 2018

On March 13, 2026, the American College of Cardiology (ACC) and the American Heart Association (AHA), together with nine other leading medical organizations, published the long-awaited updated guideline on the management of dyslipidemia. The document was released simultaneously in two flagship journals and immediately drew close attention from the medical community worldwide.
Why were the new recommendations necessary?
The 2026 guideline replaces and officially withdraws the previous 2018 guideline. Notably, the very title reflects a fundamental conceptual paradigm shift: whereas the 2018 document was called the "Management of Blood Cholesterol," the new edition emphasizes "dyslipidemia" as a whole — a term covering the full spectrum of lipid metabolism disorders, including hypertriglyceridemia and elevated lipoprotein[a].
Over the past eight years, cardiology has made a qualitative leap: new drugs have emerged, large randomized clinical trial results have accumulated, and more accurate cardiovascular risk assessment tools have been developed. According to the AHA, one in four American adults has elevated low-density lipoprotein cholesterol (LDL-C), which multiplicatively increases the risk of myocardial infarction and stroke. Atherosclerotic cardiovascular disease (ASCVD) remains the leading cause of death worldwide, which is why updating the recommendations was recognized as an urgent scientific task.
The final document contains more than 90 pages of evidence, 18 illustrative figures, and 27 tables. In this article we will analyze each key change in detail, compare the 2026 and 2018 positions, and explain the clinical meaning of each innovation.
Renaming and broader scope: from cholesterol to dyslipidemia
The first thing that strikes a reader of the new document is the change of its name. This is not merely cosmetic. The shift from "management of cholesterol" to "management of dyslipidemia" reflects a fundamental change in understanding the pathophysiology of atherosclerosis.
In 2018, therapy was primarily targeted at LDL-C — and only LDL-C. The new recommendations acknowledge that ASCVD risk is not exhausted by the level of "bad" cholesterol. Other apolipoprotein B–containing particles are atherogenic as well: triglyceride-rich particles and their remnants, as well as lipoprotein(a). For this reason, the 2026 guideline for the first time comprehensively addresses management of hypertriglyceridemia and significantly expands recommendations on Lp(a) — a risk factor that has long remained in the shadows of clinical practice.
Moreover, the document is thematically broadened: it now includes sections on children and adolescents, specific high-risk populations (patients with chronic kidney disease, HIV, diabetes mellitus, cancer), reproductive risk factors in women, and primordial prevention — that is, preventing the very appearance of risk factors in childhood and adolescence.
New risk assessment tool: PREVENT equations instead of Pooled Cohort Equations
Problems with the old calculator
One of the most resonant changes of 2026 was the replacement of the basic cardiovascular risk assessment tool. For more than a decade, US practice relied on the Pooled Cohort Equations (PCE) — equations developed for the 2013 recommendations and used in the 2018 edition. Despite their wide use, the PCE had a significant flaw: according to Blumenthal, they systematically overestimated 10-year risk of myocardial infarction and stroke by 40–50%. This led to overprescription of statins for some patients whose real benefit might not have outweighed potential harm.
The PREVENT equations: what they are and why they matter
The new standard — the AHA PREVENT equations (Predicting Risk of cardiovascular disease EVENTs) — were developed specifically for contemporary US populations and provide a more accurate and personalized risk estimate. The PREVENT equations are intended for adults aged 30 to 79 years without established ASCVD or subclinical atherosclerosis and with LDL-C levels from 70 to 189 mg/dL.
The key advantage of PREVENT is the ability to calculate not only 10-year but also 30-year ASCVD risk. This is particularly important for younger patients who may have a formally low 10-year risk but whose accumulated "atherogenic burden" over decades can lead to catastrophic consequences in middle age. Calculating 30-year risk opens the door to discussing lifetime consequences of elevated LDL-C and can justify earlier preventive interventions.
The CPR model: Calculate — Personalize — Reclassify
The guideline authors propose a convenient mnemonic — the CPR model. It includes three sequential steps:
C (Calculate) — calculate the 10-year ASCVD risk using the PREVENT equations
P (Personalize) — personalize the estimate by adding "risk-enhancing" factors not accounted for in the base formula
R (Reclassify) — if necessary, reclassify the patient using additional tools — primarily the coronary artery calcium (CAC) score
In practice this means that a clinician who obtains a baseline risk estimate is obliged to supplement it with clinical context: family history of premature ischemic heart disease, presence of chronic inflammatory diseases (systemic lupus erythematosus, rheumatoid arthritis), metabolic syndrome, obesity, diabetes mellitus, chronic kidney disease, as well as reproductive risk factors in women (early menopause, preeclampsia, history of gestational diabetes). Belonging to certain ethnic groups with higher risk — people of South Asian descent, from the Philippines — is also considered a factor that amplifies calculated risk.
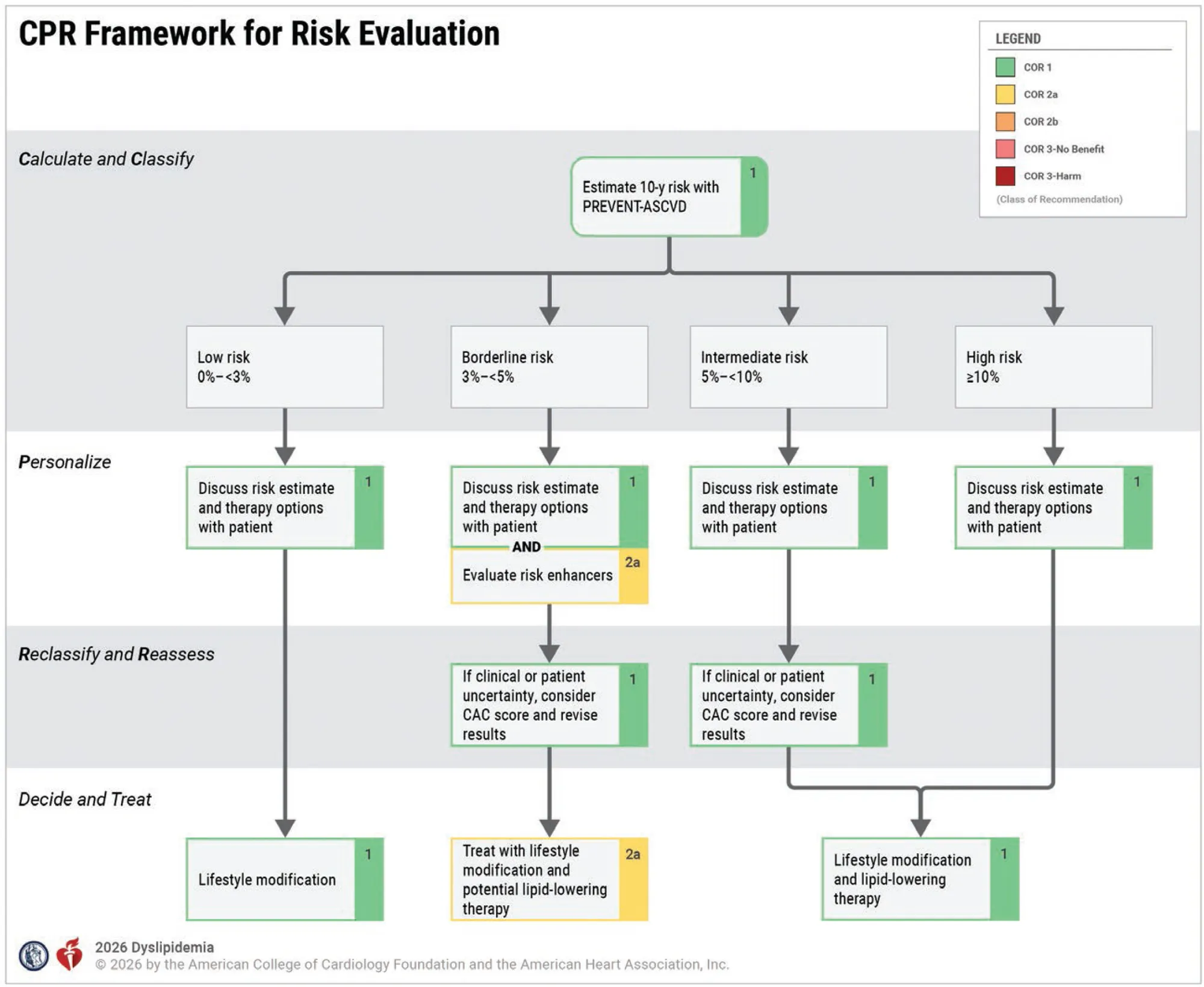
Updated 10-year risk categories
Low (< 3%) — lifestyle modification; pharmacotherapy generally not required
Borderline (3% to < 5%) — discuss the appropriateness of therapy; consider CAC
Intermediate (5% to < 10%) — LDL therapy should be considered; CAC may clarify the decision
High (≥ 10%) — lipid-lowering therapy recommended
Return of LDL-C targets: a decisive reversal
Arguably the most discussed change of 2026 is the return of specific numeric targets for LDL-C. It is important to understand this in historical context.
What happened in 2018
The 2018 guideline intentionally abandoned fixed LDL-C targets in favor of the "the lower the better" concept. Instead of specific numbers, it emphasized achieving a certain percentage reduction from baseline LDL-C: high-intensity statin therapy should achieve a reduction of ≥50%, and moderate-intensity 30–49%. This decision was criticized by practicing clinicians who need clear "targets" in real-world practice. The lack of specific numeric benchmarks complicated decision-making and assessment of treatment effectiveness.
What now: specific targets for each risk category
The 2026 guideline corrects this deficit by returning a clear system of target values tied to the risk level:
Primary prevention: borderline/intermediate risk
LDL-C target (mg/dL)< 100
non-HDL-C target (mg/dL)< 130
Primary prevention: high risk
LDL-C target (mg/dL)< 70
non-HDL-C target (mg/dL)< 100
Primary prevention: heterozygous familial hypercholesterolemia, subclinical atherosclerosis, or ≥1 ASCVD risk-enhancing factors
LDL-C target (mg/dL)< 70
non-HDL-C target (mg/dL)< 100
Secondary prevention: ASCVD, not very high risk
LDL-C target (mg/dL)< 70
non-HDL-C target (mg/dL)< 100
Secondary prevention: ASCVD, very high risk
LDL-C target (mg/dL)< 55
non-HDL-C target (mg/dL)< 85
Criteria for "very high risk" in the context of secondary prevention include: acute coronary syndrome within the past 12 months; prior myocardial infarction (apart from the aforementioned ACS); prior ischemic stroke; symptomatic peripheral artery disease; OR one major ASCVD event in combination with any of the following: age over 65 years, prior revascularization, active smoking, diabetes mellitus, heart failure, hypertension, or LDL-C > 100 mg/dL despite maximally tolerated statin and ezetimibe therapy.
It is important to emphasize that the return of numeric targets does not mean abandoning the "as low as possible" concept: the guideline explicitly states that lowering LDL-C below the specified thresholds further reduces ASCVD risk and is therefore welcomed, especially in very high-risk patients.
The role of apolipoprotein B as an additional benchmark
The new guideline also rehabilitates apolipoprotein B (apoB) as an important tool for monitoring therapy. ApoB is present on the surface of every atherogenic particle — LDL, VLDL, remnants — so its level more accurately reflects the total "atherogenic burden" than LDL-C alone, especially in patients with high triglycerides, diabetes, or when LDL-C is achieved < 70 mg/dL. At LDL-C values below 70 mg/dL, the accuracy of the standard Friedewald calculation falls sharply, and this is where apoB becomes a more reliable marker. The guideline recommends using the more accurate Martin/Hopkins or Sampson/NIH equations instead of the outdated Friedewald formula to calculate LDL-C.
Lipoprotein(a): from the shadows to the center of attention
One of the most significant innovations of 2026 is the full inclusion of Lp(a) into the routine evaluation algorithm for every adult patient. This change can be called revolutionary for American cardiology practice.
What is Lp(a) and why does it matter?
Lipoprotein(a) is a unique atherogenic particle whose level is 70–90% genetically determined and is practically independent of diet, physical activity, or most lipid-lowering drugs. High Lp(a) is an independent, causal risk factor for ASCVD not captured by standard risk calculators that operate only with LDL-C. It is estimated that about 20% of the world population have elevated Lp(a), and most of them are unaware of it.
Threshold values and clinical interpretation
The 2026 guideline introduces the following thresholds for Lp(a):
≥ 125 nmol/L (50 mg/dL) — considered a risk-enhancing factor that increases ASCVD risk by approximately 1.4-fold
≥ 250 nmol/L (100 mg/dL) — associated with at least a twofold increase in long-term risk of myocardial infarction and stroke
When elevated Lp(a) is identified, this should serve as a rationale for more intensive LDL-C lowering and aggressive control of all other risk factors.
Who and when to measure?
The guideline recommends measuring Lp(a) at least once in the lifetime of every adult. Because Lp(a) level is genetically determined and remains stable throughout life, repeat measurement is generally not required in the absence of specific clinical indications. For children under 18, cascade testing is considered if high Lp(a) is found in a parent — especially when familial hypercholesterolemia is present.
Comparison with the 2018 recommendations
In the 2018 guideline, Lp(a) was mentioned only as one of many "risk-enhancing factors" and was recommended to be measured only in equivocal cases. There was no mandate for routine testing of all adults. Thus, the shift from "measure when indicated" to "measure at least once in everyone" is a qualitative change.
Coronary artery calcium: targeted application
The coronary artery calcium (CAC) score, measured by non-contrast CT, retains an important place in the 2026 guideline, but the indications for its use have been clarified. CAC is recommended for men aged 40 and older and women aged 45 and older with borderline or intermediate ASCVD risk when there is uncertainty about initiating statin therapy. In other words, CAC is a reclassification tool rather than a routine screening test.
According to the new recommendations, the mere detection of any coronary calcium (CAC > 0) is an argument in favor of setting an LDL-C target < 100 mg/dL. At higher CAC values — depending on the absolute amount and the corresponding standardized percentile for the patient's age, sex, and race — LDL-C targets may be lowered further. Conversely, CAC = 0 allows with high probability the deferral of pharmacotherapy in intermediate-risk patients.
Compared with 2018, where CAC was already present, the concept has not fundamentally changed — rather, its role within the CPR model has been specified and algorithmized.
Lipid-lowering pharmacotherapy: statins and beyond
Statins: still the cornerstone
Statins remain the first-line pharmacotherapy across all ASCVD risk categories. The 2026 guideline does not question their evidence base but significantly expands the list of scenarios in which nonstatin medications should be added to statins.
Nonstatin agents: expanding the arsenal
In 2018, nonstatin agents were considered mainly as reserve options for patients with insufficient response to statins or statin intolerance. In 2026 their role has grown substantially. If LDL-C targets are not achieved on maximally tolerated statin therapy, the guideline recommends the following stepwise therapy:
Ezetimibe — an intestinal cholesterol absorption inhibitor; remains the first add-on step when statins alone do not achieve targets
Bempedoic acid — a new oral inhibitor of hepatic cholesterol synthesis at the ATP-citrate lyase level; particularly valuable for patients with statin intolerance
PCSK9 inhibitors (monoclonal antibodies: evolocumab, alirocumab) — injectable agents providing an additional 50–60% LDL-C reduction on top of statins; indicated primarily for very high-risk patients and homozygous/heterozygous familial hypercholesterolemia
Inclisiran — an RNA interference agent that suppresses hepatic PCSK9 synthesis; administered twice a year; promising for improving adherence, although its effect on hard endpoints (MI, mortality) is still under investigation
An important innovation: bempedoic acid is mentioned as a full-fledged alternative in the treatment algorithm — its randomized data (the CLEAR Outcomes trial) confirmed reduction in cardiovascular events, allowing it to take a place in the guideline. This drug did not exist on the market in the 2018 version.
Inclisiran: cautious optimism
Interestingly, the guideline authors take a measured approach to inclisiran: acknowledging its ability to substantially lower LDL-C, they note that data on its impact on ASCVD events are still insufficient. The ongoing ORION-4 trial should fill this gap. This is a good example of scientific honesty: recommendations do not rush to get ahead of the evidence base.
Early and lifelong prevention: the central theme of 2026
The key narrative of the new guideline is expressed in the phrase: "Lower LDL for longer" — lower LDL-C for a longer time provides incomparably greater cardioprotection than intense lowering started late. This is not just a slogan: it is supported by data showing that every additional decade of life spent with normal LDL-C substantially reduces lifetime ASCVD risk.
In this context, the guideline for the first time so clearly articulates a primordial prevention strategy — preventing the very emergence of risk factors. This includes healthy diet, physical activity, normal body weight, smoking cessation, and prioritizing healthy sleep from the earliest ages.
Hypertriglyceridemia: expanded recommendations
Unlike the 2018 guideline, which briefly addressed hypertriglyceridemia, the 2026 document dedicates an extensive section to it. This reflects growing understanding of the atherogenic role of triglyceride-rich particles and remnants.
Statins as the foundation for ASCVD risk
In hypertriglyceridemia (TG > 200 mg/dL) for patients with increased ASCVD risk or established ASCVD, statins remain the foundation of pharmacotherapy. Their ability to reduce ASCVD events is independent of baseline triglyceride levels, making them first-line agents in this context.
Prevention of pancreatitis
At very high triglyceride levels (TG ≥ 1000 mg/dL), priority shifts to prevention of acute pancreatitis. In these situations, specific triglyceride-lowering agents can be used: high-dose omega-3 fatty acids (icosapent ethyl / eicosapentaenoic acid), fibrates, niacin. New classes of drugs — apoC-III inhibitors and ANGPTL3 inhibitors — are on the horizon but require further data on cardiovascular outcomes.
Lifestyle: always at the foundation
Despite the abundance of pharmacological innovations, the 2026 guideline unambiguously states: a healthy lifestyle remains the foundation of ASCVD prevention and cannot be replaced by any drug.
1. Nutrition
A diet rich in vegetables, fruits, whole grains, legumes, lean proteins, and fish is recommended. The Mediterranean diet, the DASH diet, and plant-based diets have the most convincing evidence. Limiting saturated fats, trans fats, added sugars, and salt are mandatory components of dietary recommendations.
2. Physical activity
At least 150 minutes of moderate aerobic activity per week (or 75 minutes of vigorous activity) combined with strength training at least twice weekly is recommended. Reducing sedentary behavior itself is recognized as a significant measure.
3. Smoking cessation and weight control
Tobacco smoking is a powerful independent ASCVD risk factor and simultaneously lowers HDL-C (the "good" cholesterol). Maintaining a normal body weight (BMI < 25 kg/m²) substantially improves the lipid profile. The new guideline for the first time addresses healthy sleep as an independent cardiovascular health factor — in line with the AHA's "Life's Essential Eight" concept.
Practical algorithms
1. Primary prevention: a stepwise approach
Based on the new guideline, the following algorithm can be built for a practicing clinician in the primary prevention of ASCVD in adult patients 30–79 years old:
Step 1. Assess the basic lipid profile (LDL-C, non-HDL-C, TG, HDL-C; preferably calculate apoB when TG > 200 mg/dL or DM)
Step 2. Measure Lp(a) at least once — at the patient's first encounter
Step 3. Calculate the 10-year (and if necessary 30-year) ASCVD risk using the PREVENT equations
Step 4. Personalize risk: add risk-enhancing factors (DM, CKD, HIV, inflammatory diseases, obesity, reproductive factors, high Lp(a), ethnic background)
Step 5. If necessary (uncertainty at borderline/intermediate risk in men ≥40 and women ≥45 years), perform CAC screening
Step 6. Set the LDL-C target according to the risk category
Step 7. Start with lifestyle modification; if targets are not reached — prescribe statins, and add nonstatin agents if needed
2. Secondary prevention: algorithm
Step 1. Establish the ASCVD risk category (very high vs. not very high) according to guideline criteria
Step 2. Set the target: LDL-C < 55 mg/dL (very high risk) or < 70 mg/dL (not very high risk)
Step 3. Prescribe a high-intensity statin at the maximally tolerated dose
Step 4. If target is not achieved, add ezetimibe
Step 5. If target still not achieved, add bempedoic acid and/or a PCSK9 inhibitor
Step 6. In case of statin intolerance — consider bempedoic acid and/or PCSK9 inhibitors + ezetimibe
Step 7. Once LDL-C and non-HDL-C targets are achieved, use apoB to assess residual risk
Conclusions
The ACC/AHA 2026 guideline on the management of dyslipidemia is not merely an update of a list of recommendations. It is a conceptual restructuring of the approach to one of the key problems in preventive cardiology.
As Dr. Blumenthal said, "we know that 80% or more of cardiovascular disease is preventable." The 2026 guideline is the most comprehensive tool to date for realizing that potential.